 No More. It Ends Here.
No More. It Ends Here.Our Goals
Keep hurting the system
till we (the KrustyLads) advise you not to.
The first critical focus point
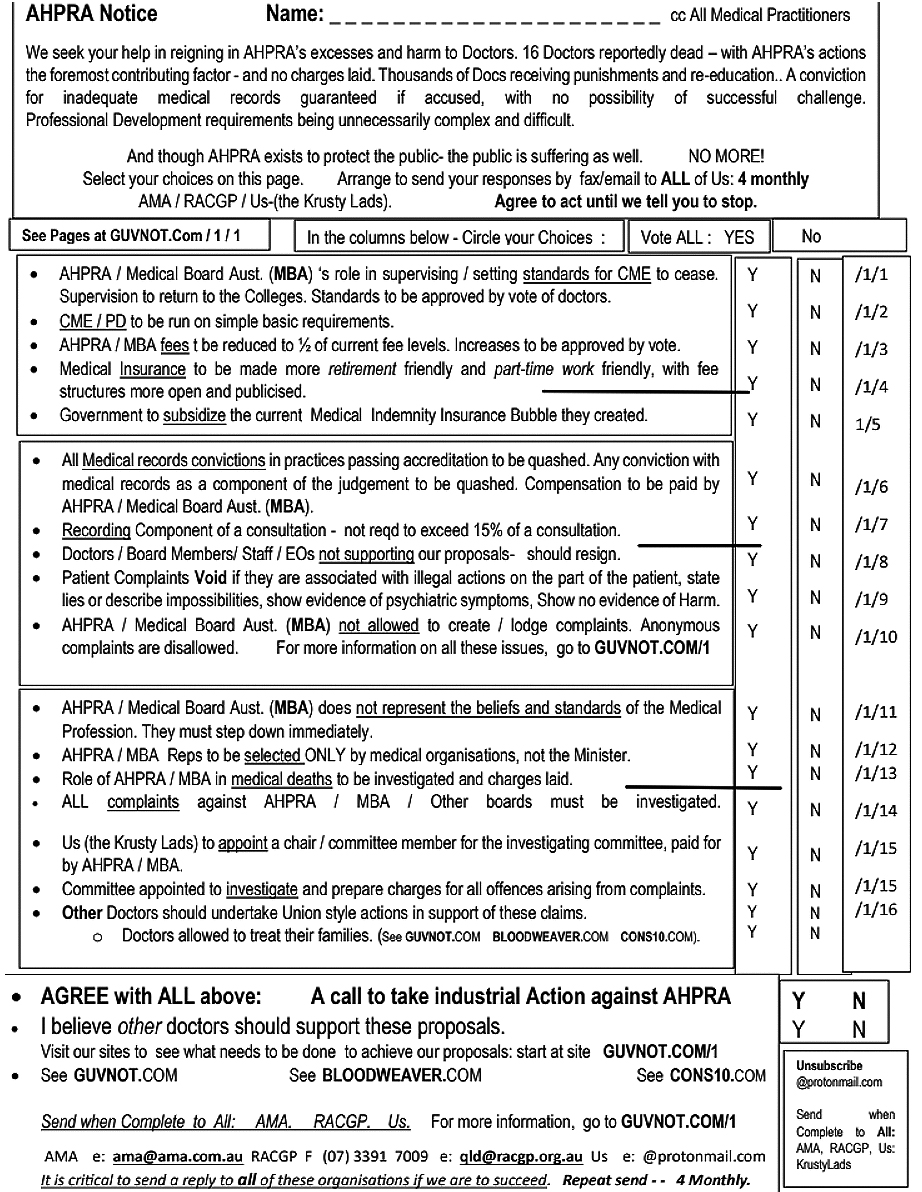
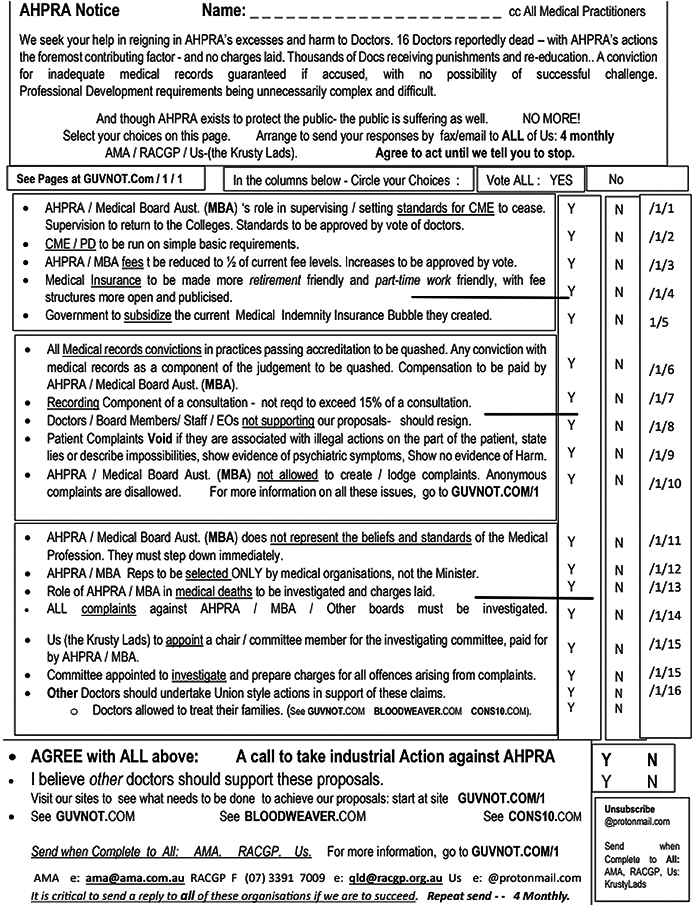
The first critical focus point of our campaign is to destroy AHPRA’s/the medical boards legitimacy and authority. We are asking you to vote that these organisations do not represent the beliefs and thoughts of the medical profession. In short they must stand down – remove themselves from office and stop working.
The Fax/ Email questionnaire is the tool by which we will achieve this. We (the Krusty Lads), ask you to support us by voting “Yes” on the questionnaire.
It is absolutely critical that you then tell everyone about the facsimile/email questionnaire.
-
Send it to the AMA
-
and the RACGP,
-
or your specialist Medical Association.
-
Send a copy to us. (Krusty Lads).
-
Please also send a copy to – other practices or doctors in your area,
other practices or doctors with whom you are familiar, -
your local Federal member,
-
and to any media representatives with whom you are familiar.
 Destruction
Destruction
Send by Fax, Email and Post.
The more the letter is replicated and forced to public awareness the more likely it will be taken seriously. So Send it to the big organisations and your friends if you believe you want things to change.
And remember: Send by Fax, Email and Post. Send to all.
The power of the questionnaire is simply based on making a choice and telling everyone about it. The survey must be distributed to as many people as possible to create a public arena awareness of our issues – to focus the community’s attention on the injustice which has become institutionalized in the medical system, and which we will no longer tolerate.
WE would also ask you to REPEAT the send-out process in FOUR MONTHS,
and then again at FOUR MONTHS.
Keep the issue on the boil.
Don't let every think its a flash in the pan that can be forgotten.
 Destroy AHPRA's Empire: Map Australia
Destroy AHPRA's Empire: Map Australia
The second critical focus
The second critical focus point of our campaign is to destroy AHPRA’s/the Medical Board’s expanding empire.
- Their role in CME/PD must end.
- We need to cut down these organisations’ financial resources (cut their payments) to stop their activities.
If there are to be "many" employees, use them to help people as human beings and as doctors do, not to act like Daleks. Obey! Obey! Obey! Obey!
- A number of the people who died, were asking for help. And look what sort of help they were given.
-
WE need to Limit AHPRA's overall powers to administrative only, with the specific powers of Supervision devolving to the specific sub-boards:
e.g. AHPRA Medical Board. This means that the specific boards can elect their own supervisory members who cannot be over-ruled by the parent body. This creates bodies akin to nation - states, not an empire.
Neutralisation: the Reaction
The third critical focus point
The third critical focus point of our campaign is to neutralise the powers that AHPRA/the Medical Boards use to hurt doctors.
The most critical of these is to use the excuse that doctors’ medical records are not adequate. The reality is that to these organisations, the medical records will never be adequate. Even if the records reproduce every thought word deed or action, it would still not be enough.
We have to set a reasonable limit on the amount of time that needs to be used to record a consultation. (We have to set standards that allow doctors to go to work and to earn a living). The most basic point of view that neutralises their stance on medical records is to say that if accreditation has said that a practice’s records including the records of its doctors are adequate, then these records are typical and representative of general practice. They are “adequate”.
The names of all the participants in an action must be included in every form or letter. It is not appropriate to simply hide behind the name AHPRA. Name the members of AHPRA, name the members of the AHPRA Medical Board and name every project officer.
This links specific people to specific actions: no one to hide behind any more.
 Investigator
Investigator
The fourth critical focus point
The fourth critical focus point of our campaign is to neutralise investigative protocols used by AHPRA/the Medical Boards.
Every doctor who attends a tribunal hearing is guilty according to AHPRA/the Medical Board. Every doctor who disagrees with the actions of AHPRA/the Medical Board has no insight according to these organisations and will be punished even more.
Statements of “inappropriate” practice are easy to come by, for AHPRA/the Medical Boards, and very difficult to defend. It is easy to say that you should have done something else more appropriate, when you do not have to prove that what you are saying is effective or safe. Even when the patients treated by doctors have good outcomes, the doctor is still judged to be practicing inappropriately. Even when the patients complain about the treatment they have received from AHPRA/the Medical Boards, no credibility is given to these claims.
AHPRA/the Medical Boards appear to be always right, even when members of the public and doctors die.
These protocols of judgment/investigation need to stop.
Doctors should not be required to confess,, especially where harm has not occurred.
Doctors should be allowed to disagree and not to be punished for disagreeing with the judgment of AHPRA/the Medical Boards.
The burden of proof should be as for the community. AHPRA/the Medical Boards should be required to “prove” – that harm has occurred. A patient complaint should always exist, specifically about any matter being investigated.
-
Complainants acting illegally, or lying or showing evidence of psychiatric symptoms in their complaint, must be dismissed.
-
AHPRA/the Medical Boards should not have the capacity to use anonymous complaints or to hide the identity of the complainant. It is the right of every person to face their accuser.
-
AHPRA/the Medical Boards need to prove that their point of view is correct and that harm would not occur as a result of their proposed actions.
-
And if harm does occur due to the actions of AHPRA/the Medical Boards, that’s called GBH: Grievous Bodily Harm and charges must needs follow against the organisation. It is only by making AHPRA/the Medical Boards fully responsible for their actions that the community and doctors will be safer and treated fairly.

So, let’s look at some of these issues: about complaints in general:
If a patient’s complaint is associated with illegal actions on the part of the patient, the complaint must be dismissed. A typical example is a patient becoming vociferous and violent, causing the practitioner to be “locked” into a room or out of their room (working space). They have in effect imprisoned or restricted the practitioner. This behaviour is not to be tolerated and the complaint must be dismissed.
Another example is for a patient to state that they have acquired medications illegally and wish the practitioner to supply them with more of these. Some of these events may even be associated with threats of violence or extortion against the practitioner. This behaviour is not to be tolerated and the complaints must be dismissed.
If a patient’s complaint contains lies or describes physical impossibilities, the complaint must be dismissed. We have seen a complaint whereby a practitioner has been accused of undertaking examination of the patient in only a couple of minutes – including taking of pulse, temperature, blood pressure, listening to heart sounds and breath sounds, looking in the ears and throat and examining the abdomen, AND writing several scripts and ordering a Urine Test.
It is physically impossible to do all these things in a couple of minutes. And yes the practitioner involved should be commended for doing the work, not asked “why are you doing this?” The complaint is thereby not unrealistic and contains an element of exaggeration and untruth - - - and must be dismissed.
If a patient shows evidence of psychiatric symptoms affecting the nature and extent of the complaint, it must be dismissed. The example we have alluded to previously is of a male doctor who was accused of being a witch by a patient. There is no justification for an inquiry into such a matter.
-
Firstly, there is derogatory language involved.
-
Secondly, the general community would believe that there is no such thing as a “witch”. If a patient’s actions suggest the presence of psychiatric illness, the complaint must be dismissed.
 Anonymous
Anonymous
All complaints must be by an identified person and the identity of the complainant must be released to the targeted individual doctor. It is not appropriate to assess anonymous complaints. In our system of justice, we have the right to face our accusers.
So, if it is AHPRA/or one of the Boards creating a complaint, it should bear asking the question as to why these organisations need to create a complaint, since no one else is complaining.
AHPRA/the Medical Boards are not allowed to write complaints on behalf of an individual. Each complainant must write and lodge their own complaint with NO input from AHPRA/the Medical Boards.
All complaints must show evidence of harm directly caused by the activity of the doctor involved. It is all too easy to disagree about what treatment or medication should or should not be used. The system relies on the statements of “professionals” , often with dubious professional qualifications, not involved in the care of the patients, to create evidence of harm. AHPRA's paid Henchmen.
The system denies credibility and authority to the statements of the patients involved. If a patient is not making a complaint of harm, it is difficult to justify an organisation inventing an accusation of harm.
The current evidentiary standard is best typified by this example: two doctors are treating 10 patients each for cancer. Dr A does everything right in the eyes of professional witnesses/colleagues. Dr B does everything wrong in the eyes of those same professional witnesses and colleagues. He has not followed the advice of the experts. However, 12 months later, all Dr A’s patients are deceased . All Dr B’s patients are well.
The Current medical standard is that Dr B would be charged with malpractice by AHPRA / the Boards . Dr A’s actions earn approval. AHPRA / the Boards even justify this stance by saying they are protecting the public.
Can anyone really be that stupid. Yes indeed. This is exactly how AHPRA/the Medical Boards undertake their investigation. Guilty at all times , and ignore any evidence which does not fit this model.
“Outcome” information should override the opinion statements of professionals employed by AHPRA / the Boards in our opinion, The only reason, you may use professional opinion is because there is often no other basis on which to make a decision. But, if there are good outcomes, how can we permit prosecutions to be undertaken by AHPRA/the Medical Boards.
Professional opinions may be a reasonable basis to judge an action, , when no other information is available. However, outcomes or consequences trump opinions on every occasion. However, this is not the current standing of the legal system in these matters.
Essentially this means if someone (often another doctor or pharmacist or health care worker), doesn’t like what you are doing, and they have complained to AHPRA / the Boards, first you will be charged and convicted for what you have done, even if what you have done has delivered favourable outcomes that the patients also agree are favourable outcomes.
Even if the actions of AHPRA/the Medical Boards deliver Unfavourable outcomes to patients.
Complaints often devolve to the fact that the patient does not like your personality or your style of consultation. This does not demand investigation. The appropriate reply should be to express some sympathy to the patient that their consultation has been difficult, identify illegalities inherent in the patient complaint ( if here are any), and direct that the patient find someone they have more understanding with. Not to proceed to crucify the doctor in question.
The Twin tablets of law : not one for each of us
The fifth critical focus point of our campaign
The fifth critical focus of our campaign is to make the organisations AHPRA/the Medical Boards , realise that they are required to follow the law as well.
-
They must not kill doctors. ( I can't believe I actually need to write this down as a valid and necessary achievement, and that a campaign needs to be undertaken to achieve it).
-
They must not injure patients.
-
They must not breach privacy laws.
-
They must not threaten people in the community who work with doctors.
-
They are responsible for harm ; e.g. GBH (Grievous Bodily Harm) they have caused.
They are required to follow the law as are we all. Any of us who are involved in a patient death, undergo a significant heart search and assessment of our actions and their effects. If someone has died, we would all in our human nature try to act never to allow such a scenario to occur again.
AHPRA/the Medical Boards have however caused doctors deaths. These organisations must be investigated for "Manslaughter". They are the primary contributory factor to the deaths occurring.
And AHPRA/the Medical Boards show no ability to self-assess or to reflect on their role in death and destruction. They do not consider their role in contributing to the death of a doctor and try to act not to allow this to happen again.
After a doctor died, they allowed deaths to occur again, and again, and again, and again, and again, and again, and again, and again, and again, and again, and again, and again, and again, and again, and again.
And these are the deaths we know about.
There are probably other doctors who have taken their own lives due to the actions of AHPRA/the Medical Boards as well. We know of more.
There are probably even patients who have taken their lives as a result of the actions of AHPRA/the Medical Boards .
There must be an investigation and laying of charges for all of these events against the members of AHPRA/the Medical Boards.
Remember, if a doctor assists a patient who wishes to die, to take their life – this is a crime.
How can it be that AHPRA/the Medical Boards can force a doctor against his will to take his life – and this is accepted and normal.
No more.
Again – investigate, lay charges through solicitors and force the system to charge AHPRA/the Medical Boards for crimes against the community.
The system of thuggish inhumanity perpetrated by AHPRA/the Medical Boards is so entrenched, that it may even be necessary for people and especially doctors giving evidence against AHPRA/the Medical Boards, to be required to give evidence in camera, (incognito).
Death to the Daleks. Or else Obey! Obey! Obey! Obey! till its your turn.
 Undemnity Indemnity
Undemnity Indemnity
The Sixth critical focus of our campaign
The Sixth critical focus of our campaign is to adjust Medical Indemnity Issues which make it difficult for doctors to work. The government subsidy for low earners does not translate to savings by the community due to what we perceive as the incompetence of the insurer.
I think 3% is a more realistic maximum fee as a percentage of income to charge practitioners, with the proviso that there can be a number of modifiers available for “at risk” doctors. Premiums charged by medical indemnity organisations should be limited to 3% of gross earnings. Errors in billing by medical indemnity organisations should be punished. (For example, billing annual premiums as well as monthly premiums, as well as refusing to supply the indemnity subsidy).
There are a few basic equity issues that are essential for medical practice.
Indemnity Fees for each profession and each level of earnings need to be publicized annually, IN FULL.
For example, in general practice we should be able to see a list of fees charged by indemnity providers for doctors earning: less than $50,000 PA, $50,000- $100,000 PA, $100,000-$200,000 PA, $200,000 to $350,000 PA, $350,000-$500,000 PA, and greater than $500,000 PA.
We should be able to see a list of modifiers that increase the cost of insurance.
Every doctor should know what to expect and when.
Reducing working hours by definition means reduced income. It is unreasonable to expect part-time doctors to pay indemnity fees approaching 1/3 of their income – even if it is to be repaid eventually in a year or so if they complain loud enough.(and probably not if they don’t complain persistently and unendingly). Doctors need to maintain some ability to work into retirement, that is not impacted by excess indemnity fees.
 Changing Leadership Roles
Changing Leadership Roles
The Seventh critical focus
The Seventh critical focus of our campaign is to make the organisations AHPRA/the Medical Boards change their roles and activities.
AHPRA needs to become an essentially powerless administrating overlooking the activities of a number of specialty medical and allied health boards – of each individual profession.
The Specific Medical Boards or Allied Health Boards / Nursing Boards need to become the specific agents supervising each individual profession. The organisations are hiding behind each other currently.
Members of each Board must be community or Industry appointed members with experience in their industry. Not some political hack given an AO (Office of the Order of Australia), for services to some political party. As an adjunct, any community member bearing Honours on a Board that is involved with community deaths, must be stripped of their Honours. Since when do we reward killers.
Community members cannot be allowed to act on a professional board. They do not have any experience with how things work in each industry. As a doctor, I do not think I should sit on the Board of Nursing, so why should some inexperienced community member.
Every complaint processed by one of the boards must contain – not the name of the board – but the actual name of the members of the board were responsible for the complaint’s progression. We should be able to identify the Guilty parties at any step in the dealings of these organisations with the medical or general community.
Action such as “Immediate Actions” – must have a set expiry date when initiated. I would suggest three months is more than adequate time for the board to progress to an inquiry. It is of course not reasonable to undertake an immediate action unless there is an undeniable basis of evidence allowing such an action to occur. So the evidence must be here already.
Any doctor affected by such an action must be paid a wage/compensation, until such complaint is heard and processed formally.
The time taken by AHPRA/the Medical Boards to progress a complaint must be consistent with the time allowed to the doctor to defend himself or herself. Currently AHPRA/the Medical Boards take years to progress a complaint and then limit the time available to defendants to a couple of months at most, when the same things took them years to organise. ( Alternately, do things differently by a new protocol).
There must be an organisation which looks at failed actions by AHPRA/the Medical Boards. The need for compensation must be assessed and if necessary compensation paid to doctors affected by the actions of AHPRA/the Medical Boards.
There must be an organisation separate to AHPRA/the Medical Boards with the capacity to investigate complaints against these organisations and with the capacity to undertake disciplinary action on AHPRA/the Medical Boards.
 In Conference
In Conference
The Final and Eighth focus of our campaign
The Final and Eighth focus of our campaign is to create a mechanism whereby the legislation governing the medical community is altered. There is no justice available at Tribunals or the PSA as many doctors have discovered.
The system over the years has changed legislation to make it progressively easier to Convict doctors accused of wrongdoing. Doctors deserve the same legal rights as other members of the community- not just the right to be raped by the establishment. We are hoping that doctors use the Bloodweaver group mechanism to push for legislative change
And that’s Us.
Keep hurting the system
till we (the KrustyLads) advise you not to.
WHAT TO DO
We are asking for support to limit AHPRA’s scope
and activities against medical practitioners.
1 in 3 practitioners can expect to have an education/mentoring/supervisory activity imposed on them within the next 10 years.
In practices I have worked, up to 50% of doctors have significant stories to tell.
I have heard stories of practitioners undertaking suicide or retiring permanently to avoid the harassment and sanctions.
No Appeal is possible against AHPRA decisions and often Medical Defence won’t fund an appeal either.
We have chosen a different direction for our campaign.
Our Story: GUVNOT.COM
To Help Us: see ContactUs.html
See Guvnot/2/2
See Guvnot/Actions
See Guvnot/1/16
Our Basic Actions
- Give a copy of this Fax/Email to every doctor in your practice.
- Send us your email address so we can keep you updated: guvnotcom@proton.me
- Visit our Site and decide to do something : GUVNOT.COM,, CONS10.COM
There are many ways and many choices available. I am sure something for everyone.
See Guvnot/2/2
See Guvnot/Actions
See Guvnot/1/16
- Basic Actions to do now: Send the fax / email / mail to
RACGP / AMA / ACCRM (cc Us - the KrustyLads as well).
(We have some basic forms you can use at GUVNOT.COM/FORMS.)
Tell them you are interested in supporting this action. You want these organisations to do something.
- More You can do : (We have some basic forms you can use at GUVNOT.COM/FORMS.)
- Send a fax or email to / State or Federal Health Minister,,
- Send a fax or email to the media. ).
- Tell Us your story if you have one. guvnotcom@proton.me
- Send a fax or email to notify colleagues who may be interested .: Just refax or email this page.
- See Guvnot/2/2
See Guvnot/Actions
See Guvnot/1/16 - ContactUs.html
Guvnot.com tells you about the many different ways that can help to win this political action.
Cons10.com tells you how change your consulting style to hurt them, not yourself.
Choose to do something. No One need ever know if you are worried about consequences (Covert Action).
Choose to do something. (Overt Action). Help us to do something,
or organise to do something as well.
 Docs gather ‘round, cause the stakes are so high.
Docs gather ‘round, cause the stakes are so high.
Keep hurting the system
till we (the KrustyLads) advise you not to.
Do the Survey online: preferably. Go direct to survey
The Fax/Mail/Email Form: send 4 monthly to all of us to remind everyone that its still an issue. Otherwise the issue just gets buried by time and by being ignored.
Copy of this form as full-size JPG, PDF, DOCX
{kind=link}
Copy of this form as full-size JPG, PDF, DOCX
Do the Survey online: preferably.
Go direct to survey
 We Want You
We Want You